Why Doctors Don't Like Medicare Advantage: The Reimbursement Math Patients Don't See

-
Last Updated July 17, 2026
Your doctor says they're "no longer accepting" your Medicare Advantage plan. Or maybe they haven't said it yet, but they've started nudging you toward Original Medicare at every visit. You're not imagining it. Across the country, doctors and hospitals are dropping MA plans, and the reasons come down to money, paperwork, and a payment system most patients never see.
This isn't an argument against Medicare Advantage. Millions of seniors get solid coverage and extra benefits through MA plans. But understanding why your doctor might resist these plans gives you better footing when it's time to choose or renew one.
The 90% Rule: How MA Carriers Make Their Margin
Here's the number that matters most: Medicare Advantage plans often reimburse doctors at roughly 90% of what Original Medicare pays for the same service. That 10% gap might sound small, but for a busy practice seeing dozens of Medicare patients a day, it adds up fast.
The math works like this. CMS (the Centers for Medicare & Medicaid Services) pays a per-member, per-month capitation rate to each MA insurance carrier. The carrier then negotiates payment rates with doctors and hospitals. Those negotiated rates are almost always lower than what Original Medicare would pay directly.
Doctors who accept Original Medicare get paid on a fee-for-service basis with published rates. There's no middleman negotiating the price down. With MA plans, the insurance company sits between the government payment and the doctor's check, and that company needs to fund its operations, pay for extra benefits like dental, vision, and OTC allowances, and still turn a profit.

Why do doctors not like Medicare Advantage plans?
If you ask a doctor I don't think you'll ever get a straight answer, but the reality is that in a lot of cases with Medicare Advantage they get reimbursed 90% of what they would get reimbursed from original Medicare. The good thing for a doctor is that original Medicare offers a lot more flexibility on treatments, and the bad thing about Medicare is that it offers a doctor a lot more flexibility on treatments. While Medicare Advantage covers the same services as original medicare, the Medicare Advantage plan likely has more protocols in place to cut down on waste and fraud than does original Medicare, such as prior authorization and referrals. Original Medicare doesn't have these restrictions, but is also one of the main reasons why it's projected to be insolvent by the year 2033. Despite the restrictions and pre-authorization, some studies do show that people on Medicare Advantage can have an adjusted life expectancy 9 to 15% longer than people on original Medicare because of the coordination of care involved with a Medicare Advantage plan.That 90% figure isn't universal. Some plans pay closer to Original Medicare rates, especially in competitive markets where carriers need to attract providers. Others pay significantly less. The variance depends on the carrier, the region, and how much leverage a particular health system has during contract negotiations.
For smaller independent practices without bargaining power, the math often doesn't work. A solo physician or small group can't absorb a 10-15% revenue cut on their Medicare patient panel and keep the lights on. That's why you'll notice it's often the smaller offices that drop MA plans first, while large hospital systems with negotiating muscle keep accepting them.
Prior Authorization: The Number One Complaint from Doctor Offices
Ask any physician's office staff what they dislike most about Medicare Advantage, and you'll get one answer before they even finish the question: prior authorization.
Under Original Medicare, if your doctor says you need an MRI, a referral to a specialist, or a particular procedure, it generally just happens. The doctor orders it, you get it, Medicare pays its share.
Under most MA plans, the insurance carrier requires the doctor's office to submit paperwork proving the service is medically necessary before it can be performed. This process can take days for routine requests and weeks for complex ones, even with 2026 rules requiring faster turnaround times. For urgent care situations, the wait can feel intolerable for both the doctor and the patient.

Why do doctors not like Medicare Advantage plans?
Some doctors aren’t big fans of Medicare Advantage because it can create extra work and limit their flexibility. Many plans require prior authorizations before patients can get tests or treatments, which slows things down and adds paperwork. Doctors may also get paid less than with Original Medicare, and sometimes claims are denied or delayed. On top of that, the networks can be more restrictive, which means doctors can’t always refer patients as freely. All of this can make the care process feel more complicated than it needs to be.The administrative burden is real and measurable. Doctors' offices hire additional staff just to handle prior authorization requests, appeals when those requests get denied, and the back-and-forth with insurance company reviewers. That overhead cost comes straight out of the practice's revenue, on top of the already lower reimbursement rates.
When a prior authorization is denied, the doctor faces a choice: perform the service anyway and risk not getting paid, or delay your care while they fight through the appeals process. Neither option sits well with physicians who entered medicine to treat patients, not to argue with insurance adjusters.
This is also why understanding how prior authorization works before you enroll in an MA plan can save you real headaches down the road. Not all plans require prior auth for the same services, and some carriers have streamlined the process more than others.
Star Ratings as a Reimbursement Lever
Most seniors know that Medicare Advantage star ratings exist. Fewer realize how directly those ratings affect what their doctor gets paid.
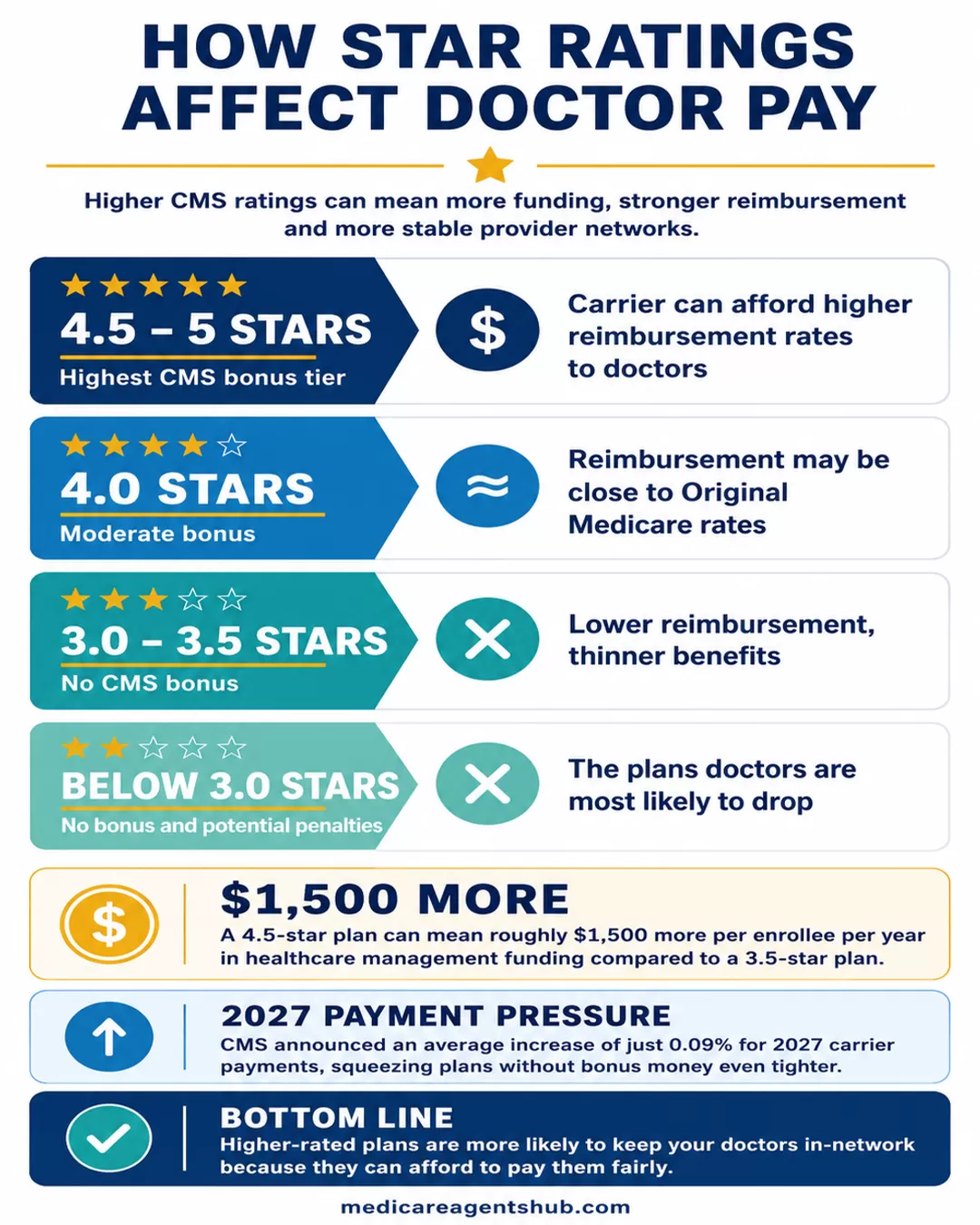
CMS assigns every MA plan a star rating from 1 to 5 based on quality measures: patient satisfaction, health outcomes, customer service, and more. Here's where it gets interesting for doctors. Plans rated 4 stars or higher receive bonus payments from CMS. That extra money flows into the plan's budget, which means the carrier has more to spend on provider reimbursement and benefits.
| Star Rating | CMS Bonus Payment | Impact on Doctor Pay |
|---|---|---|
| 4.5 - 5 Stars | Highest bonus tier | Carrier can afford higher reimbursement rates |
| 4.0 Stars | Moderate bonus | Rates may be close to Original Medicare |
| 3.0 - 3.5 Stars | No bonus | Lower reimbursement, thinner benefits |
| Below 3.0 Stars | No bonus, potential penalties | Doctors most likely to drop these plans |
A 4.5-star plan can mean roughly $1,500 more per enrollee per year in healthcare management funding compared to a 3.5-star plan. That difference directly affects how much the carrier can pay providers. Doctors know this. The ones paying attention to their reimbursement checks can tell which plans are rated higher just by looking at the payment amounts.

Why do doctors not like Medicare Advantage plans?
CMS has just released its 2026 payments to carriers for 2027. The average increase for contracted carriers is 0.09%, and some counties in Washington are getting 0.02%. Doctors want more money, and the carriers are being paid less. Plans that are 4 Star or higher get paid more and can pay doctors more. A 4.5-star plan receives more money than a 3.5-star plan. Doctors do not want to accept average-rated plans because they receive lower reimbursement. A 4.5-star plan will cost around $1,500 more per year for healthcare management. Naturally, they can pay more to the doctor. The best action you can take is get a high-rated plan or a supplement plan. Carriers are reducing benefits. I believe you will see larger reductions in WA next year, including OTC, Dental, and other benefit types. Doctors get paid less under PPO plans; in Spokane, Multicare and Providence are no longer accepting PPO plans.This is why picking a high-rated plan isn't just about bragging rights or slightly better customer service. It can determine whether your doctor stays in your plan's network next year. When CMS announced an average increase of just 0.09% for 2027 carrier payments, that squeezed already-thin margins even tighter for plans that don't earn bonus money through strong star ratings.
If you're comparing MA plans and see a 3-star plan with flashy benefits next to a 4.5-star plan with slightly less generous extras, think about what's happening behind the scenes. The higher-rated plan is more likely to keep your doctors in-network because it can afford to pay them fairly. That trade-off between visible benefits and provider stability is one of the most overlooked factors in plan selection.
What to Ask Your Doctor Before Picking an MA Plan
Knowing the mechanics puts you in a better position to have an honest conversation with your doctor. Here are the questions that actually matter.
"Which MA plans do you currently accept, and are you planning to drop any next year?"
Doctors' network contracts renew annually. A doctor who accepts your plan today might not accept it in January. Ask directly, especially during the fall before Annual Enrollment Period. Most offices know by September or October which contracts they're renewing.
"Have you had issues with prior authorization on my plan?"
Your doctor's front office staff deals with this daily. They know which carriers approve requests quickly and which ones drag their feet. If your doctor's office tells you a specific plan is a nightmare to work with, that's worth factoring into your decision, because administrative friction translates directly into delays in your care.
"Would you recommend I consider Original Medicare with a Supplement instead?"
Some doctors will say yes immediately. Others will give a more nuanced answer. Either way, it's worth understanding their reasoning. If your doctor strongly prefers Original Medicare patients, it's usually because they've had too many experiences where MA plan restrictions interfered with the care they wanted to provide.
"If you drop my plan mid-year, what are my options?"
Network changes don't only happen at the start of the year. Contracts between carriers and providers can end mid-year, leaving you scrambling.

What happens if my specialist leaves the network in the middle of the year?
Several things will happen. If you have appointments after their departure, you will be considered out of network and pay a higher copay. You may or may not be notified by your provider and/or doctor's office. Claims before any departure are safe, will still be processed in network even if they are submitted afterwards. Lastly, you may be able to request a Continuity of Care Exception if you are in active treatment or have a long standing relationship with the specialist.Hope this helps!
The possibility of mid-year network disruption is one of the strongest arguments for working with a licensed Medicare agent who can help you evaluate plan stability, not just benefits. An agent who knows your local market can tell you which carriers have the most stable provider networks and which ones have a history of losing doctors.
The Bigger Picture: This Isn't About Picking Sides
None of this means Medicare Advantage is a bad product. For many seniors, the zero-premium structure, out-of-pocket caps, and extra benefits that Original Medicare doesn't offer make MA the smarter financial choice. The point is that the system has real tensions built into it, and those tensions show up in your doctor's waiting room.
Doctors want to be paid fairly and practice medicine without fighting an insurance company over every imaging order. Insurance carriers need to manage costs to keep premiums low and benefits attractive. CMS is trying to keep the whole system solvent while encouraging quality through star ratings. All three goals are legitimate. They just don't always align.
As a patient, your job is to pick a plan with open eyes. Check the star rating. Ask your doctor the hard questions. Look at the plan's prior authorization requirements before you enroll, not after you need surgery. And if your doctor does drop your plan, know that you have options, whether that means switching back to Original Medicare or finding a higher-rated MA plan that your providers will stick with.